August 2024 Research Insights & Updates

The number of patients identified with RVCL has more than tripled in the last few years. The good news is that Dr. Jonathan Miner, Associate Professor of Medicine at the University of Pennsylvania, and our network of collaborators are making meaningful progress in finding a cure for RVCL. Today, we’re pleased to share an update on our website highlighting the Latest Research Insights.
We aim to continue providing regular research updates to our sponsors and supporters. Here are a few of our latest updates:
Breast Cancer Risk in Women with RVCL / RVCL-S
The latest video relates to our recent discovery that RVCL is associated with high-risk of early-onset breast cancer in women. We found that RVCL is a DNA Damage Syndrome, which means that the abnormal TREX1 protein causes injuries to chromosomes, leading to organ damage (mimicking radiation injury) and increased risk of cancer. Patients and families should be aware of this, as it may have implications for cancer screening. Please reach out to us if you have questions.
Collaboration Across Four Continents
The second video introduces you to our network of collaborators at the University of Michigan, around the United States, and also in Japan, France, Scotland, Australia, and beyond. These partners are helping us develop therapies. We also want to update that we have preliminarily confirmed that our gene therapy works in the livers of mice (after intravenous injection). We will have a long way to go, but our fruitful collaborations across four continents are creating a path toward personalized therapies:
WATCH BOTH VIDEOS HERE
Where Are We Today?
The task before us is challenging, and we cannot predict the timing. However, in just three short years, we have already achieved a great deal. We’ve managed to engineer mice to express the human TREX1 gene, and have determined a path to fix the mutation in adult mice, bringing us closer to a potential cure.
We are diligently working to develop small-molecule drugs. In collaboration with the University of Michigan, expert medicinal chemists are creating small-molecule drugs that bind the TREX1 protein and block its DNA-damaging effects. We have screened seven billion drugs and narrowed it down to a few hundred, with a lead compound already identified. We hope these drugs will eventually be taken as pills and that they will slow disease progression. The Clayco Foundation and others are accelerating this work by supporting us and engaging a contract research organization to synthesize new compounds for more rapid testing.
Our partnerships and shared goals—among patients, families, trainees, and staff in the lab, and our international collaborators—are making all of this possible.
Please get in touch with us if you need anything, and feel free to share these updates with your families and friends or anyone we might have inadvertently left off our list.
Netosis – Is it a cause of RVCL?
Netosis is the act of neutrophils “shooting out” their DNA and histones as a ‘web-like’ structure, usually to catch bacteria. These Neutrophil Extracellular Traps, or NETS, are quite bactericidal and inflammatory, and improperly controlled Netosis has been linked to various disorders such as Cystic Fibrosis and COVID. A reasonable hypothesis would stipulate that erroneous NET formation may be involved in initiating or exacerbating RVCL.
Experiments have now demonstrated that neutrophils from RVCL patients are less prone to Netosis (via spontaneous measure or by stimulation), and follow-up studies concluded that Netosis is not related to the pathology or severity of RVCL. While this conclusion is subject to change pending further research and scientific advancement, it looks to rest here as of today.
While this would seem to be “negative” data that does not inform us of a particular way to treat or combat RVCL, it is just as critical. Many rocks need to be looked under when studying such a complex disorder, and any and every mechanism eliminated as a potential culprit only makes it easier to narrow in on more valuable pathways. We are proud to continue supporting such research and welcome all results as they help us define a focused picture.
Exploring RVCL-Mutated TREX1 Activities in the Nucleus of Cells

Exploring RVCL-Mutated TREX1 Activities in the Nucleus of Cells: Interplay with Nuclear Envelope (NE) Rupture, DNA Damage & Innate Immune Sensors
The pathology in RVCL is speculated to stem from dysregulation in DNA damage, innate immune activation or cellular senescence. TREX1 mutations in RVCL lead to the generation of a truncated form of TREX1 due to a frameshift (TREX1-fs). While wild-type (WT) TREX1 is normally located at the endoplasmic reticulum, TREX1-fs adopts a pan-cellular localization and is present in the nucleus. TREX1-fs retains DNAse activity, including in vivo, but it is unable to damage DNA in micronuclei. The potential contribution of DNA damage and innate immune activation in the primary nucleus during RVCL is unclear. Overall, the activities of TREX1-fs in the nucleus remain incompletely understood. Here we propose to investigate the nuclear pool of TREX1-fs in new contexts of DNA damage, senescence and innate immune activation.
It is known since its identification that, unlike WT TREX1, TREX1-fs is a pan-cellular protein at steady state. However, the impact of TREX1-fs on the nucleus is largely unknown. Recent findings prompt us to pay renewed attention to nuclear TREX1-fs: first, the finding that WT TREX1 mediates DNA damage in the nucleus after NE rupture, and second, the appreciation that cells contain a nuclear pool of cGAS. These recent findings constitute an opportunity to investigate TREX1-fs in yet unexplored contexts. They signify that RVCL could result in part from currently unappreciated effects of TREX1-fs in the nucleus.
By shifting the focus to the nuclear pool of TREX1-fs, our proposal provides an innovative concept. Furthermore, NE rupture can be induced by mechanical forces that are applied through microfabricated devices or through the use of specific modulators, which represent innovative and multi-disciplinary approaches. Finally, our expertise in nuclear cGAS and the wide range of tools that we have developed constitute innovations to study TREX1-fs.
 Dr. Nicolas Manel, Ph.D.
Dr. Nicolas Manel, Ph.D.
Director of Research
Institut Curie
Dr. Nicolas Manel Ph.D. is a virologist with an immunological focus with years of experience in dealing with insidious diseases, such as HIV, and how they stimulate different signaling pathways in various cell types. Recently, his lab has successfully studied how several viruses with envelope viral particles transmit the second messenger cGAMP to activate immune response in target cells and that dendritic cells protect themselves to cope with the infectious nature of viruses. His lab also revealed that innate immune sensors are active in cells of adaptive immunity and identified mechanisms that limit the intracellular immune response to self DNA. His lab investigates the regulation, function and application of innate immunity with the goal to discover the molecular mechanisms that enable the immune system to distinguish self from non-self inside cells. They study HIV, other viruses and auto-immunity and development of the immune system, now applying their expertise to RVCL research.
Developing a Microfluidic Model of RVCL

Developing a microfluidic model of RVCL
Dr. David Hunt, M.D., Ph.D.
Retinal vasculopathy with cerebral leukoencephalopathy (RVCL) is a devastating and untreatable systemic monogenic microangiopathy caused by frameshift mutations in TREX1, a 3′-5′ DNA exonuclease. Pathogenic monoallelic mutations are restricted to the C-terminus region of TREX1 which tethers the enzyme to the endoplasmic reticulum (ER), where it plays an important role in degrading immunostimulatory nucleic acid species such as ssDNA. At a pathological level RVCL is primarily an endotheliopathy, affecting the microvascular beds of multiple organs including the brain, the eye and kidneys/liver/bone. How loss of TREX1 ER tethering causes endothelial disease is not yet established. Understanding RVCL pathogenesis requires physiological models which recapitulate the central microvascular hallmark of disease, but microangiopathy is not widely seen in Trex1 frameshift mouse models. As such there is an unmet need to develop human microvascular models of disease. Here we propose to develop a “microvasculature on-achip” model of RVCL, with an overall aim of understanding the molecular and cellular basis of RVCL, and finding treatments. Thus, we will aim to i) generate and characterize endothelial cells with RVCL mutations and ii) To establish a microfluidic system for the study of RVCL microvessels.
Developing human microfluidic systems has the potential to accelerate therapeutic discovery for RVCL by linking cellular disease phenotypes to physiological dysfunction of microvessels. As our knowledge of the cellular consequence of C-terminal TREX1 frameshift mutations increases, it is important to test candidate therapeutic interventions in a physiologically relevant system. RVCL is an ultra-rare disease with limited clinical trial opportunities, so developing stringent models for preclinical testing of candidate drugs is critically important. The development of a microfluidic model would, therefore represent a significant advance in identifying potential therapies for RVCL.
At present, there are no published microfluidic model systems based on RVCL mutations available to researchers. Our proposed project has the potential to identify therapeutic targets and also to provide a resource for the research community through the generation of RVCL mutant endothelial lines, together with optimized microfluidic approaches. All reagents and protocols will be made freely available to accelerate the wider RVCL research effort.
 Dr. David Hunt, M.D., Ph.D.
Dr. David Hunt, M.D., Ph.D.
Professor
The University of Edinburgh
Dr. David Hunt M.D., Ph.D is a Wellcome Trust Clinician Scientist and Honorary Consultant Neurologist who leads clinics and research in the field of brain inflammation. He trained in medicine at Cambridge, London and Basel. His PhD research at Cambridge University was in the field of developmental neuroscience and neuroinflammation. In 2009 he moved to Edinburgh where he completed his neurological training and established a Wellcome Trust-funded laboratory to study the molecular basis of neuroinflammatory diseases such as multiple sclerosis and lupus. He currently serves as the Chair of Neuroinflammation Medicine and runs a weekly clinic for patients with complex neuroinflammatory diseases.
David’s research group is focused on trying to identify the molecular pathways which drive inflammation. His team adopts a multidisciplinary approach, using stem cell-based models and genetic models based around neuroinflammatory diseases. His work has identified how innate immune mechanisms such as the type I interferon pathway can drive aspects of brain disease and how this might be targeted in future clinical trials. He has led the development of patient-focused clinics for the bedside-to-bench study of neuroinflammation, with particular emphasis on ‘neglected’ inflammatory disease of the brain such as lupus and RVCL.
The Phenomenon That is Cellular Senescence

Cellular Senescence is the phenomenon in which cells permanently arrest (a.k.a. cell growth ceases), which is a normal aging mechanism. While the lack of cellular senescence may at first glance seem a boon to anti-aging efforts, the lack of these signals and this pathway would interfere with healthy aging as the body knows it and could cause significant problems.
Studies have now demonstrated that TREX1 would seem to be directly linked to the normal process of cellular senescence (aging), and that mutations in the TREX1 gene seem to lead to erroneous regulation of senescence-related genes. It was also noticed that many of the TREX1 mutation samples were deficient in histone counts, and this could be related to improper chromatin folding (an underlying issue in several age-related diseases). Therefore, it is possible that this dysfunctional senescence may be an underlying mechanism of RVCL – and, thus, something to target.
For more information pertaining to this scientific discovery, contact us here.
As more RVCL patients are identified, and research continues, we are optimistic that more studies will lead to more breakthroughs and, eventually, a strong therapeutic option. Stay tuned for more updates, and visit us at RVCL.org!
Using Drosophila Genetics and Optical Coherence Tomography to Advance RVCL Research

Using Drosophila Genetics and Optical Coherence Tomography to Advance RVCL Research
Retinal vasculopathy with cerebral leukoencephalopathy (RVCL) is a rare genetic disorder that manifests mainly in middle age individuals; in most patients death occurs 5 to 10 years after onset.1 The disease is caused by mutated TREX1 gene; for example a frameshift at val235 (V235fs) results in truncated protein, which may cause misregulation of oligosaccharyltransferase (OST) complex leading to immune system disbalance.2 The underlying mechanisms of disease pathogenesis are still unknown. Our lab would like to join the effort led by the RVCL Research Center at Washington University to investigate the mechanisms of RVCL by developing an innovative and efficient RVCL disease model based on Drosophila melanogaster.
In this program, we will develop and characterize various fly models related to the RVCL disease, including fly TREX1 (CG3165) knock-down and knock-out, and human TREX1 WT and V235fs mutant rescues. Fly models can significantly speed up the research in mammalian systems and help to eliminate false positive leads. These fly models are suitable for the advanced research of the RVCL disease throughout the fly lifecycle, and will provide a valuable toolbox for genetic screening of drug targets to combat the RVCL disease.
Leveraging the unmatched set of genetic and biochemical tools offered by the Drosophila models and the non-invasive in vivo OCT imaging tools developed in our group, we will establish an innovative interdisciplinary research platform to perform a series of new experiments, providing insights into conserved mechanisms on the RVCL disease and explore potential therapeutic strategies that is not feasible before. Of course, modelling human diseases in flies has its limitations; but research coordination between Drosophila and mammalian systems can intensify the RVCL cure development.
 Dr. Chao Zhou, Ph.D.
Dr. Chao Zhou, Ph.D.
Associate Professor
Washington University in St. Louis
Chao Zhou’s research interests are in optical coherence tomography, a growing technology used to perform high-resolution cross-sectional imaging using light. He has multiple grants funded by the National Institutes of Health, the National Science Foundation, and other federal and private sources. He holds multiple U.S. and international patents for his inventions, and has published dozens of articles in peer-reviewed journals as well as several book chapters. He is an Editorial Board Member for Communications Biology, and associate editor for IEEE Photonics Journal, Journal of Biomedical Optics and Medical Physics.
Retinal Multimodal Imaging in RVCL
Retinal multimodal imaging in RVCL
Dr. Rajendra Apte, M.D., Ph.D.
Retinal vasculopathy with cerebral leukoencephalopathy (RVCL) is a rare autosomal dominant vascular dementia and retinopathy. Histologically. RVCL causes a disease that resembles premature aging of small blood vessels. Patients with RVCL begin to develop retinal and cerebral disease around age 40, that ultimately leads to blindness, dementia, and premature death around age 50. Retinal findings include capillary obliteration, micro aneurysms, branch retinal artery occlusions, ischemia. and secondary proliferative retinopathy, similar to other diseases such as diabetic retinopathy. Although ischemic central visual acuity loss has been described in RVCL patients, this only measures the central one degree of visual function. The effects of RVCL on global retinal structure and visual function have not been well characterized. We propose to perform multimodal retinal imaging and visual testing in order to non-invasively quantify the effects of RVCL on the neurosensory retina.
There is a paucity of data on how RVCL affects the neuronal and vascular structure of the neurosensory retina at various stages of disease. Although visual acuity information is available, effects of RVCL on visual field, contrast sensitivity, visual circuitry, and on the individual layers of the retinal vascular plexuses including the inner and outer retinal vasculature, as well as the choroidal vasculature are unknown. Using non-invasive multimodal imaging, we will be able to i) establish a baseline for how RVCL affects comprehensive visual function; ii) whether the retina can be a non-invasive biomarker for RVCL severity and iii) to be able to assess in the future how therapies may improve retinal structure and function.
We will use non-invasive technologies including Goldmann visual field testing to map the peripheral and central visual fields. Using dark adaptometry we will measure the sensitivity of retinal photoreceptors and the ability to dark adapt, a metric that if impaired has significant functional consequences for patients. Optical coherent tomography (OCT) will facilitate an almost histologic examination of the layers of the neurosensory retina and quantify the effects on both inner and outer retinal neurons. Recent advances in OCT have allowed the development of a specialized technique called OCT angiography (OCT-A). This imaging technique is also non-invasive and allows examination of the inner, middle and outer retinal vasculature as well as the choroidal vascular plexus with high resolution cross-sectional imaging. The advantage of OCT-A is that it allows high resolution imaging of the macular vasculature, the very central part of the retina responsible for precise vision. It will complement our findings from wide field dye-based angiography. No additional dye injection is needed for OCT-A. Retinal auto fluorescence will capture any effects of vascular alterations and non-perfusion on the retinal pigment epithelium. The multimodal approaches highlighted below will enhance our clinical understanding of how both the vasculature and the neuronal circuitry in the retina is affected by RVCL and will likely provide a) molecular disease insights and b) establish a detailed baseline for future natural history and therapeutic response studies.

Dr. Rajendra Apte, M.D., Ph.D.
Professor
Washington University in St. Louis
Dr. Rajendra Apte M.D., Ph.D. is the Paul A. Cibis Distinguished Professor of Ophthalmology and Visual Sciences. His areas of specialty include age-related macular degeneration, diabetic retinopathy and retinal vascular diseases, retinal surgery, macular holes and retinal detachments. He has further research efforts into innate immunity and the immune effector mechanisms in the retina; oxidative stress and cell death; models of developmental angiogenesis and neovascularization; inflammation and photoreceptor survival, and macular degeneration. He also serves as the vice chair for the Innovation and Translation program
Optical Coherence Tomograph Study Used to Analyze Retinal Layers of RVCL Patients
Earlier this year, the publication Spectral Domain Optical Coherence Tomography in Retinal Vasculopathy With Cerebral Leukoencephalopathy and Systemic Manifestations: A Monogenic Small Vessel Disease came out in the Journal of Neuro-Ophthalmology by Dr. Irene de Boer in the Terwindt lab in the Netherlands. And though a mouthful of a title, this publication adds to our knowledge base about RVCL and, importantly, ways to improve early diagnosis.
Because several organs are affected in RVCL, including the eyes, analyzing retinal anatomy has become increasingly used as a biomarker for earlier diagnosis. In this study, Optical Coherence Tomograph (OCT) was used to analyze multiple retinal layers of RVCL patients (TREX1 mutation) compared to control, healthy individuals. OCT provides a noninvasive cross-sectional visualization of optic disc and macula, and a difference was observed in this study.
As still very little about OCT in RVCL patients is known, the authors decided to focus on one overall measurement of the peripapillary region (peripapillary retinal nerve fiber layer, pRNFL) thickness as well the macular region (total macular volume, TMV). The findings were that RVCL patients had significant reductions in the thickness of these layers, and it was important to look at both because pRNFL thinning has been observed in other hereditary diseases but without concurrent macula thinning. This study demonstrated retinal thinning in patients with RVCL in the peripapillary and macular area, even when the funduscopic examination was normal.
As the authors state, it is vital for patients with RVCL that they are recognized by ophthalmologists. Not only is ophthalmological monitoring critical, but neurological monitoring and treatment for anemia, hypertension, and kidney failure might be necessary. If the diagnosis is not recognized, this can lead to unnecessary, possibly harmful, biopsies (including, but not limited to, brain and kidney biopsies). Furthermore, misdiagnosis can have severe treatment implications. The diagnosis of RVCL should be suspected in adult patients of middle age presenting with vascular retinopathy and/or focal or global neurologic deficits, particularly in a positive family history of retinopathy or neurological diseases. Given that patients often present with vision loss, the ophthalmologist should be cautious in cases of vascular retinopathy without an apparent etiology.
More in-depth scientific information can be found here: https://pubmed.ncbi.nlm.nih.gov/34334759/
De Boer et al. Spectral Domain Optical Coherence Tomography in Retinal Vasculopathy With Cerebral Leukoencephalopathy and Systemic Manifestations: A Monogenic Small Vessel Disease. J Neuroophthalmol. 2022. PMID: 34334759
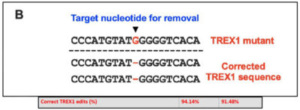
Can Correcting the TREX1 Mutation Reverse RVCL?

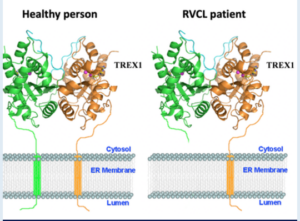
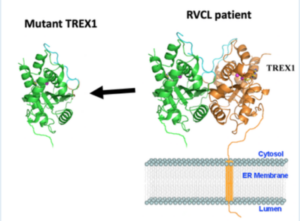
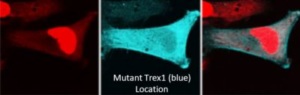
Genetic mutation leading to disease is not a new discovery or phenomenon, and many have heard of such afflictions as Down Syndrome, Cystic Fibrosis, and Huntington’s Disease to name a few. And though RVCL is far rarer, it too is a disease caused by aberrant mutations in the patient’s genetic signature. Specifically, it is typically caused by a random mutation in the transmembrane “anchor” domain of the TREX1 gene which leads to its ‘free-floating’ in the cell (rather than tight regulation at the cell membrane). If this genetic code could be restored, might it be possible to reverse and correct the RVCL disease?

In 1987, the first hints of the Clustered regularly interspaced short palindromic repeat (CRISPR)-Cas system was beginning to be identified. These CRISPR sequences are widespread in archaea and bacteria, and were first discovered in the bacteria E. Coli during genetic studies. It was then noticed that they seem to always be coordinated with the Cas proteins, proteins that can cleave and remove specific (mutated) DNA sequences. While the studies since the foundational discoveries have been impressive and deep, the punchline today is that the system (of an RNA guide to a DNA sequence of interest + an attached protein capable of cutting it out to allow for correct DNA repair) appears useful in treating genetic disorders. Recent publications have highlighted its usefulness in different diseases, including Transthyretin amyloidosis1, Sickle Cell2, and soon to be more3,4. Thus, the question must be asked: Could this CRISPR-Cas system be utilized to repair mutant TREX1 and restore RVCL patients to a healthy stature?
Recent in vitro (a.k.a. in “Petri dishes”) experiments with TREX1 mutant cells and the CRISPR-Cas system has revealed a greater than 90% “gene correction rate” with a less than 10% off-target effect. And though this is only in the lab today and requires much more effort to reach a point of legitimate therapeutic potential, this scientific validation is crucial. Might RVCL be treatable and even possibly curable at its foundational misstep in the TREX1 gene? Time and research will tell…stay tuned!
- Gillmore, J, et al. CRISPR-Cas9 In Vivo Gene Editing for Transthyretin Amyloidosis. NEJM 385:493-502. 2021.
- Frangoul H, et al. CRISPR-Cas9 Gene Editing for Sickle Cell Disease and B-Thalassemia. NEJM 384:252-260. 2021.
- Lu L, et al. Application of CRISPR/Cas9 in Alzheimer’s Disease. Frontiers in Neuroscience. 2021.
- Abdelnour, S et al. The Potential of CRISPR/Cas9 Gene Editing as a Treatment Strategy for Inherited Diseases. Frontiers in Cellular Development and Biology.